Context
Community
Healthcare and society face several major challenges in the coming decades. This year, more than a quarter of the total government expenditure will go to healthcare. The Scientific Council for Government Policy has calculated that if we do not act now, healthcare costs will triple between now and 2060, which is, of course, completely unaffordable. Secondly, there is a double challenge due to the increasing aging population on one hand and staff shortages on the other. We are living with more elderly people compared to the working population, often with chronic illnesses or multiple conditions. Currently, 1 in 6 people in the Netherlands works in healthcare, and this will rise to 1 in 4 if we do nothing, which is not feasible. Moreover, due to high workloads, administrative burdens, and lack of autonomy, absenteeism is only increasing, and more people are leaving healthcare. Thirdly, there is increasing social inequality and, consequently, health disparities. Recently, it became clear that in the Netherlands, people with lower education and income levels live, on average, 15 years less in good health, influenced by various factors such as living conditions, knowledge, and skills. All this already leads, and will certainly lead further in the future, to an increasingly severe healthcare bottleneck if we do not structurally reorganize or, better said, transform the healthcare system.
In the northern provinces, there are additional specific challenges. Due to the migration of youth from rural areas, aging will increase further, but the potential for informal care will also decrease, thereby increasing pressure on the healthcare system. Residents in rural areas, including Groningen, Friesland, and Drenthe, often have a lower socioeconomic status, poorer health, higher healthcare consumption, and less trust in government policy compared to urban areas. There is a relatively high level of physically demanding labor, which can lead to musculoskeletal complaints, including osteoarthritis.
The above challenges were among the reasons for drafting the Integrated Care Agreement (IZA), a joint multi-year plan describing a major transition in healthcare and its organization. The cornerstone of the IZA is appropriate care: value-driven, centered around and with the patient, at the right place, physically when necessary, and digitally when possible. Appropriate care focuses on health instead of illness and emphasizes prevention.
Additionally, the Ministry of Health, Welfare, and Sport outlined several missions in the 2024-2027 mission document, which will guide the (organization of) healthcare in the coming years. These are:
- Central Mission: By 2040, all people in the Netherlands will live at least five years longer in good health, and the health disparities between the lowest and highest socioeconomic groups will have decreased by 30%.
- Mission 1: By 2040, the disease burden caused by unhealthy lifestyles and unhealthy environments will have decreased by 30%.
- Mission 2: By 2030, healthcare will be organized 50% more (or more often) in people’s own living environments, together with their (social) network.
- Mission 3: By 2030, the proportion of people with chronic illnesses or lifelong disabilities who can participate in society to their desired extent and ability will have increased by 25%.
- Mission 4: By 2030, the quality of life for people with dementia will have improved by 25%.
- Mission 5: By 2035, the population will be better protected against socially disruptive health threats.
 Figure 1. Missions, outlined by the Ministry of Health, Welfare, and Sport.
Figure 1. Missions, outlined by the Ministry of Health, Welfare, and Sport.
UMCG: Koers25 & Koers30
Within the UMCG, the aforementioned challenges have been among the driving forces behind the development of Koers25 and soon Koers30, with the mission: Together, we push boundaries for a sustainable future of health. The UMCG is a high-tech, specialized knowledge institution with deep roots in society and a strong connection to the University of Groningen. It serves as a unique engine of innovation in the fields of prevention, care, research, education, and training. Our work is meaningful to patients, citizens, partners in government and business, health insurers, students, and researchers worldwide. This gives the UMCG a special position and responsibility at the regional, national, and international levels.
The vision of the UMCG is to provide groundbreaking and high-quality complex care for and by people in an integrated healthcare landscape. Moreover, in all our core tasks, we aim to act as an engine of innovation regionally, nationally, and internationally. The three priorities – Healthy Ageing, a people-centered and value-driven approach, and data-informed working – guide our actions in all our core activities. In everything we do, at every level of the organization, we keep these priorities in focus. We achieve this through five pillars:
- Integrated networks for prevention, care, research, and education
- Discovering and innovating diagnostics and treatments
- Future-oriented education and training
- The UMCG as a sustainable and inspiring employer
- Being an agile and results-driven organization
Department of Anesthesiology
Anesthesiological care encompasses comprehensive care for patients in the pre-hospital and perioperative phases, as well as (ambulatory) pain management. The focus is on safety, pain management, and maintaining physiological stability. The field integrates knowledge of anatomy, physiology, pharmacology, and psychology for the administration and management of anesthetics and other medications, addressing both acute and chronic pain.
Anesthesiology is characterized by interprofessional and interdisciplinary collaboration and plays a crucial role throughout the healthcare chain, from pre-hospital and perioperative (acute) care to pain management and monitoring, both in-hospital and outpatient.
The Department of Anesthesiology contributes to the ambitions of Koers25/Koers30 and the needs of society, both now and in the future, through research and innovation.
Mission
Improving perioperative health and pain care through insight, innovation, and connection.
Vision
- We are a (inter)nationally leading research group focused on restoring, preserving, and improving homeostasis in our patients, aiming to prevent/reduce tissue and organ damage that leads to diminished postoperative and post-intervention quality of life and function.
- We develop and implement new technologies for research, prediction, diagnostics, treatment, education, evaluation, and monitoring throughout the (perioperative) care process.
- We design and implement, where possible, personalized (pharmacological) interventions to optimize patients’ health status and prevent and/or treat damage/complications. This is not only quantitatively but also qualitatively oriented toward quality of life and patient satisfaction. We de-implement interventions that add no value for the patient.
- We work value- and data-driven, multi- and interdisciplinary, and transmurally, connecting with patients throughout their entire care journey and focusing on effective prevention.
- Our research is sustainable and aims to reduce the burden/environmental footprint for people, society, and the climate.
- We disseminate knowledge in (inter)nationally leading journals within an open science culture.
- We patent knowledge in collaboration with private partners, ensuring that scientific results are rapidly translated into tangible care for patients.
- We hold an inspiring and leading role in care, research, education, and innovation, connecting stakeholders across (Northern) Netherlands.
This requires a multidisciplinary approach and the expertise of various professionals. Our research team includes clinical care professionals in Anesthesiology (anesthesiologists, anesthesia assistants, physician assistants, nurses) as well as pharmacologists, engineers, medical technologists, health scientists, paramedics, and data scientists, and where relevant, collaborates with other healthcare providers and experts outside the field of Anesthesiology.
Strategy: Redefinition of research lines; the 4 domains
Currently, the Department of Anesthesiology at the UMCG has defined 5 research lines and appointed 5 professors in the areas of pharmacology, neuroscience, hemodynamics and monitoring, pain, and educational innovation.
To further increase our impact in the region and the scientific field, and to fully utilize our broad expertise, these strong substantive lines will be firmly anchored in a research agenda that aligns with societal and professional challenges for the coming decades. This agenda compels us to further develop our field, reduce silos, and stimulate collaboration. The proposal is to work towards the following complementary domains in 2024:
- Monitoring, Technology, and Personalized Care
- Developing and implementing technology for continuous monitoring of vital functions and physiological processes to maintain accessible and high-quality care.
- Enhancing decision-making through the use of data to remotely monitor and treat patients’ (vital) functions, enabling personalized care choices both in and out of the hospital, and developing new care pathways, prevention interventions, (AI) algorithms, smart applications, and individual alerts in collaboration with other research groups and public-private partnerships.
- Continuously integrating knowledge from these projects into our decision models and care processes.
- Building transmural networks and investigating how to establish effective care chains for the right care in the right place, from prevention to aftercare or palliative care.
- (Perioperative) Organ Damage, Inflammation, and Recovery
- From molecule/cell to society: Conducting research to gain new knowledge on the personalized (patho)physiology of organ damage and recovery at the molecular/cellular, organ, and system levels—both experimental, translational, and clinical. Contributing to damage limitation, optimal patient recovery, and improved quality of life.
- Investigating both short- and long-term outcome parameters and understanding what matters to individual patients.
- Optimizing (post-intervention) pain management to prevent the development of or progression to chronic pain and the associated loss of function and quality of life.
- (Perioperative) (Pharmacological) Therapeutic Interventions
- Developing new forms of (personalized) interventions, both in and outside the hospital, that enhance perioperative/peri-intervention health. Central to this is the consideration of whether interventions are delivered at home, near the patient, or in the hospital.
- Investigating which interventions do not contribute to improved perioperative/peri-interventional health and de-implementing them.
- Pharmacological optimization: Studying the pharmacology of existing and new drugs necessary to restore and maintain the patient’s homeostasis during the perioperative process. This involves applying pharmacometric principles, artificial intelligence, and advanced drug delivery technology to achieve a personalized pharmacological therapeutic strategy.
- Innovation in Education
- Passion and talent in transition: Researching the dynamics of transitions and social capital as well as mechanisms to nurture passion, talent, and professional identity development. Integrating these insights into our educational programs to foster a supportive and sustainable learning environment.
- Curiosity: Researching and developing education that stimulates curiosity. This includes creating personalized education in areas such as e-learning, peer-assisted learning, interprofessional education, and incorporating technology and theater into skills education. Aiming for a facilitative, inclusive, and connective education system for a future-proof professional in a changing healthcare landscape.
- Stress and well-being: Investigating the perception, impact, and response to stress, promoting well-being, and building resilience. This includes diagnostic qualitative and quantitative research into areas such as ‘speaking up,’ self-awareness, and the impact of new technologies. The focus extends to organizational and systemic improvement with the goal of ensuring sustainability for the future.
- Education as the driving force for change: Driving necessary changes to bring our results, innovations, and advancements into daily practice. Sharing insights with others and collaborating with various knowledge institutes in the region. Education is a domain interwoven with the other domains.
These domains are not confined silos but complement and strengthen each other.
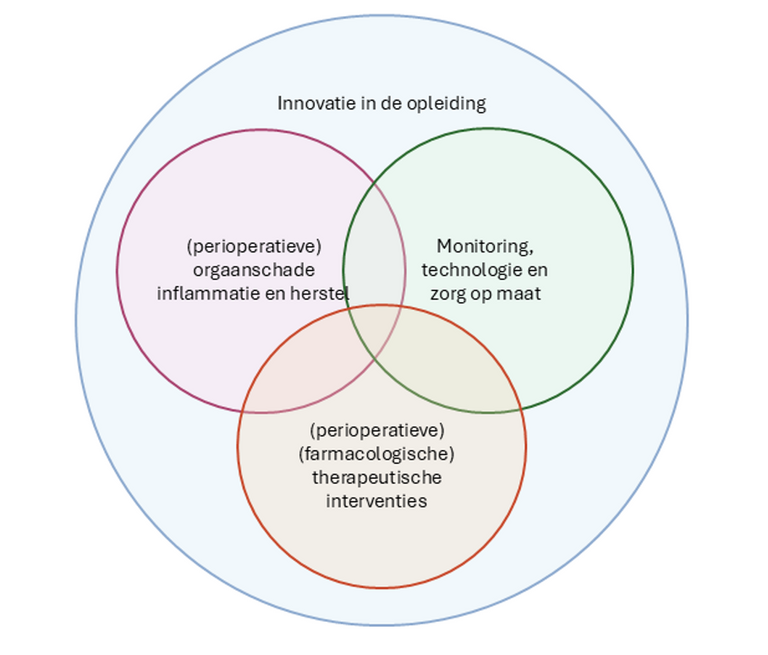 Figure 2. Research domains within the Department of Anesthesiology.
Figure 2. Research domains within the Department of Anesthesiology.
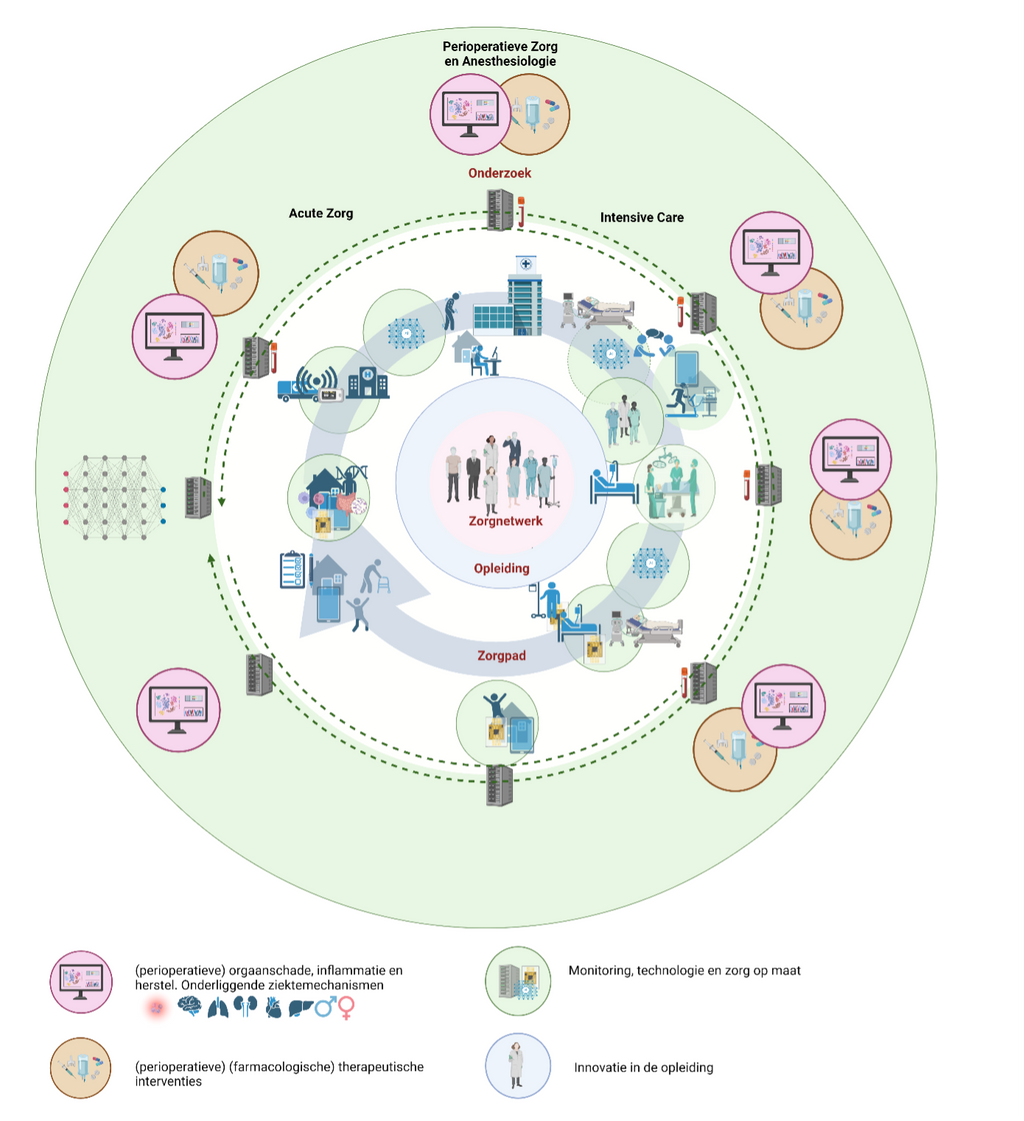 Figure 3. Our research agenda is integrated into our care process and education.
Figure 3. Our research agenda is integrated into our care process and education.
Monitoring, Technology, and Personalized Care: During the various phases of the patient journey (pre-hospital, outpatient clinic, surgery, postoperative, long-term), data and biomaterial can be collected. This data originates from health apps, wearable sensors, electronic health records, and other platforms. We use this data to develop decision models and (further) advance (monitoring) technology supported by artificial intelligence. We then implement these developments back into the care process in collaboration with the patient and other healthcare providers within the perioperative care network.
Perioperative Organ Damage, Inflammation, and Recovery: During the various phases of the patient journey (pre-hospital, outpatient clinic, surgery, postoperative, long-term), we collect biomaterial and data to study personalized underlying (patho)physiological mechanisms of organ damage and recovery. This knowledge flows back into our decision models and therapeutic interventions.
(Perioperative) (Pharmacological) Therapeutic Interventions: During the various phases of the patient journey (pre-hospital, outpatient clinic, surgery, postoperative, long-term), we develop and study new forms of (personalized) interventions and pharmacological optimization.
Innovation in Education: We invest in our social capital by researching professional identity development, the perception, impact, and response to stress, promoting well-being, and building resilience. We aim for a facilitative, inclusive, and connective education system for a future-proof professional in a changing healthcare landscape.
Prerequisites
To be successful and sustainable, several prerequisites are set concerning staffing, funding, research organization, and job satisfaction.
- Staffing: Each domain has a designated domain lead. The aim is to build a healthy, future-proof academic structure consisting of professors, associate professors, assistant professors, postdocs, and PhD candidates to ensure sufficient impact. Since we do not work in silos, this ambition is collectively managed, and staffing is flexibly deployable.
- Funding: Funding is essential for research. Each domain will seek appropriate external funding to remain viable. For social innovation, programs such as the IZA (Integrated Care Agreement) and TAZ (Future-Proof Labor Market in Healthcare and Welfare) offer opportunities. Organizations like InvestNL also provide options. These projects are mission-driven, working toward a pre-defined vision for the future. Subsidy bodies such as NWO, NWA, ZonMw, Interreg-EU, SNN, and Top Sectors will also be utilized. Efforts will focus on forming and maintaining consortia to enhance the department’s visibility and increase success in securing research funding.
- Organization of Research: Setting up and conducting research requires time and money, both of which are limited. Therefore, a business-like perspective is essential. In addition to centrally organized research support, we aim for project-based embedding of necessary research support within our research office, ensuring projects are financially viable. The research office will further professionalize and align with the API cluster. Since research is a fundamental task of our academic department, all staff members can be involved in research. The deployment of the research office aligns with the entire research group, with priority given to funded studies with execution obligations.
- Job Satisfaction: Collaboration is essential to enhance the impact of research. By working together, we can not only achieve more success in designing and conducting research but also help each other and individuals excel. Trust is crucial for successful collaboration. By celebrating each other’s successes, we can achieve more together. The following principles guide us:
- We talk with each other, not about each other.
- We are transparent about our projects so that it is clear who is working on what.
- There is formal and informal space for connection and brainstorming.
- We are open about ambitions and (career) opportunities.
- We actively promote (talent) development. Experienced researchers mentor younger researchers.
- We help each other, leveraging our specific knowledge/expertise for tasks such as writing grant applications or statistical analysis.
- We care about each other’s well-being and employability.
- We inspire, inform, and involve the entire department regarding our research projects.
- We actively collaborate with partners within and outside the UMCG and introduce each other to valuable contacts in our personal networks.